

What can this method achieve?
In patients with severe autoantibody-mediated autoimmune diseases, pathogenic antibodies have to be rapidly deactivated or removed from the blood. Tryptophan immunoadsorption (TRIA) has been used for over 30 years for targeted removal of such antibodies, both for acute in-clinic situations and in outpatient settings for chronic autoimmune diseases.
Established in numerous clinics and treatment centers
Neurologists are often the initial points of contact who identify the indication for treatment. DIAMED immunoadsorption treatments are performed in cooperation with nephrologists (specialists in extracorporeal blood treatment), intensive care specialists, or independently. Extensive clinical data is available for the diseases listed below.
What diseases tryptophan immunoadsorption can be used for?
Immunoadsorption can be applied for:
Neurology
- Multiple sclerosis (MS)
- Neuromyelitis optica (NMOSD)
- Autoimmune encephalitis
- Myasthenia gravis (MG)
- Guillain-Barré syndrome (GBS)
- Chronic inflammatory demyelinating polyneuropathy (CIDP)
Nephrology
- Goodpasture syndrome
- Focal segmental glomerulosclerosis (FSGS)
- Systemic lupus erythematosus (SLE)
…and numerous further rare antibody-mediated autoimmune diseases.
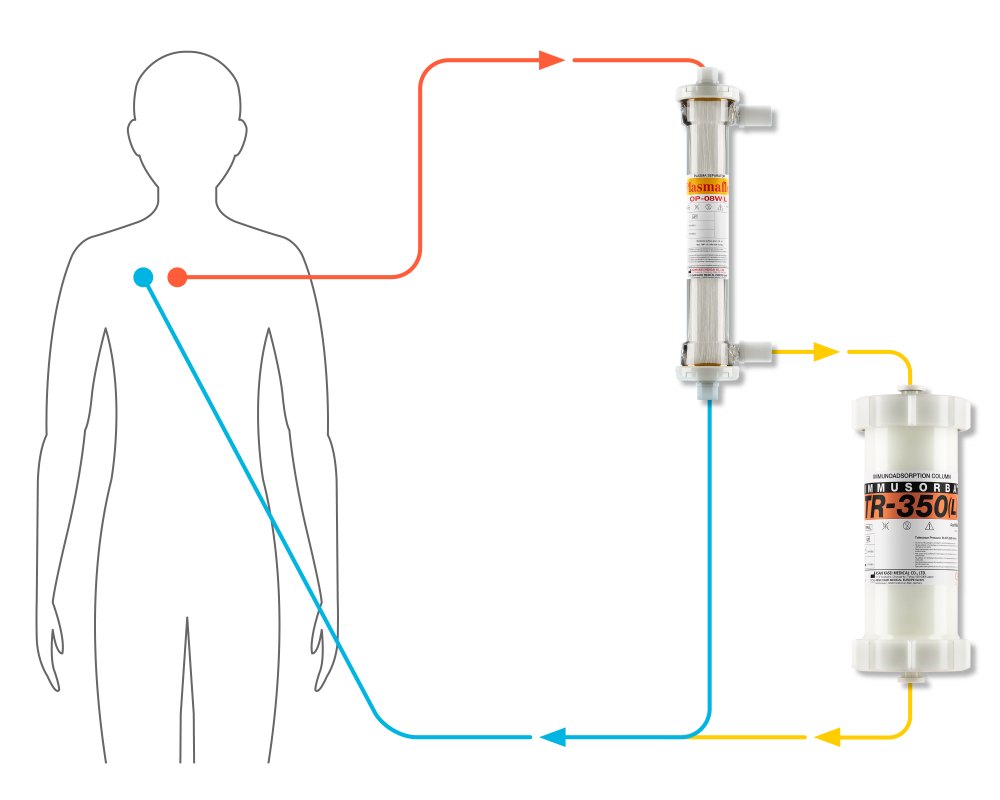
How does immunoadsorption with single-use columns work?
In immunoadsorption, a plasma separator is used to separate the patient’s blood into a cell-rich fraction and plasma. Autoantibodies from the plasma are captured in the Immusorba TR-350 column. This adsorber contains the ligand tryptophan, which provides targeted adsorption of the various IgG subclasses as well as IgMs. Once purified in this way, the patient’s own plasma is returned to the body and re-combined with the cell-rich fraction. For each treatment, physicians use a fresh new adsorber – hence the term “single-use column”.
Plasma exchange is the non-specific alternative to selective immunoadsorption. In this treatment method, all of the plasma is discarded, including valuable plasma proteins such as coagulation factors. The replacement solution that is reinfused into the patient – human albumin or donor plasma – can cause intolerance reactions. In comparison, users describe tryptophan immunoadsorption as being significantly better tolerated and associated with fewer side effects.
Up to 2.5 liters of plasma are treated during one tryptophan immunoadsorption treatment – a significantly smaller volume than with plasma exchange. Nevertheless, TRIA shows comparable effectiveness and may even starting showing effects sooner.
Typically, a series of six immunoadsorption treatments are conducted over a period of about ten days.
How long do the effects of immunoadsorption treatment last?
It has long been known that the effects of tryptophan immunoadsorption can persist for months after the treatment series is complete. This is explained by its unique three-stage effect:
- Immunoadsorption treatment directly removes autoantibodies from the blood.
- This causes a pulse-like redistribution of immunoglobulins from the extravascular space. About 50% of IgGs are found here, and they now pass over to the blood.
- The immunoadsorption triggers a multifaceted cellular immunomodulation process. This effect has been shown to persist for a longer period of time, and may explain the persistence of clinical improvements over a period of months.
How effective is tryptophan immunoadsorption?
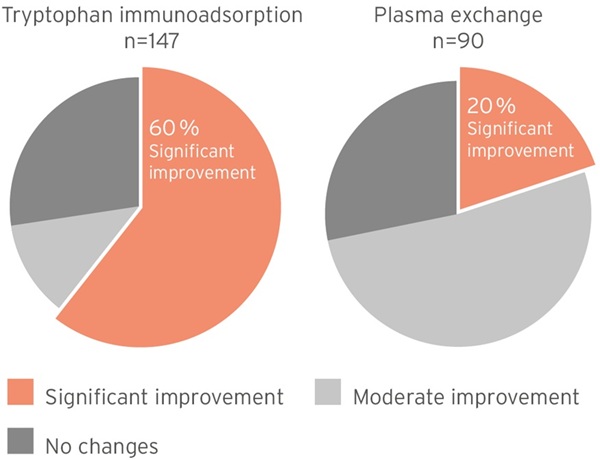
Multiple sclerosis
Patients with multiple sclerosis have responded well to immunoadsorption. In a documented case collection of 147 patients, six of ten patients with severe relapses that had previously not responded to steroids showed significant clinical improvement. Right: Results for plasma exchange.
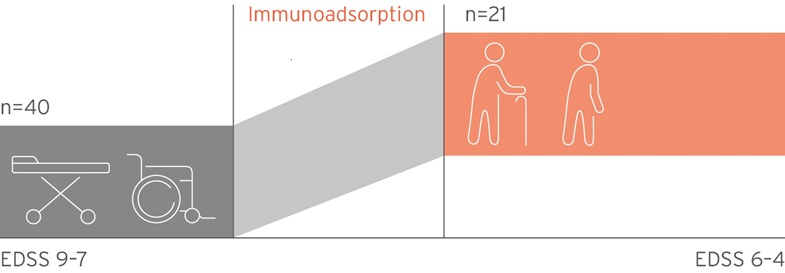
Suitable for severe cases
After a series of tryptophan immunoadsorption treatments, 52% of previously bed-ridden or wheelchair-bound MS patients were able to improve their mobility.
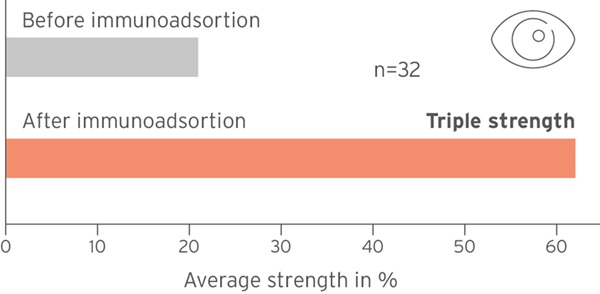
Improving visual acuity in optic neuritis
If the optic nerve is acutely inflamed - for example during an attack of multiple sclerosis or neuromyelitis optica disease - vision can deteriorate abruptly, even leading to blindness. Four out of five patients were able to see significantly better again after treatment with tryptophan immunoadsorption (5.4 treatments on the mean).
Autoimmune encephalitis
Tryptophan immunoadsorption is indicated for severe forms of autoimmune encephalitis. In a pilot study, 11 of 13 patients treated with tryptophan immunoadsorption showed rapid clinical improvement. Many different autoantibodies are already known to be implicated in this disease, and new ones continue to be discovered. Tryptophan immunoadsorption is increasingly being recommended as a first-line treatment.

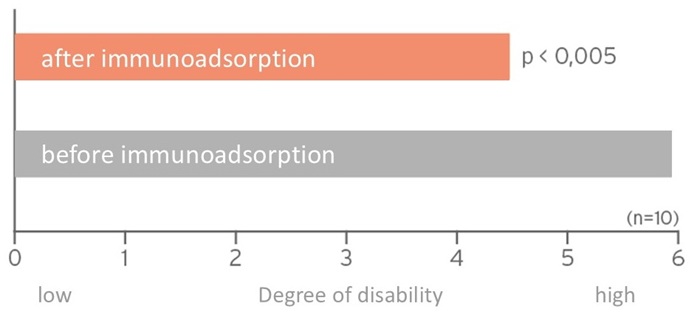
Chronic inflammatory demyelinating polyneuropathy (CIDP)
Tryptophan immunoadsorption shows significant effectiveness in patients with severe CIDP that does not respond to drugs. Nine of ten patients had significantly fewer symptoms after treatment. CIPD patients’ degree of disability was reduced after immunoadsorption therapy.
Tryptophan immunoadsorption proofs long-term effectiveness
For many diseases, the exact pathogenic autoantibodies involved are not known. Users therefore prefer both to work selectively, and also to use a broad adsorption profile. The specific structure of the tryptophan ligand allows Immusorba TR-350 to effectively remove both IgM and IgG antibodies. IgG subclasses 1, 3 and 4 are removed just as effectively as IgMs.


Cost reimbursement, coding & documentation in Germany
Over 100,000 treatments have been conducted to date. For purposes of the DRG supplemental reimbursement, tryptophan immunoadsorption is reimbursed under OPS code 8-821.0 on a hospital-specific basis.
Fee-per-case catalog: Coding for immunoadsorption with non-regenerable columns uses OPS code 8-821.0 “Immunoadsorption with non-regenerable column to remove immunoglobulins and/or immune complexes”.
The cost will be reimbursed via the hospital-specific Supplemental Reimbursement ZE13.
- 2023 InEK (Hospital Reimbursement Institute) fee-per-case catalog (in German)
- BfArM (German Federal Institute for Drugs and Medical Devices) OPS code catalog (in German)
Supporting documents for claim submissions: Correct and complete documentation of each treatment is essential. We’re happy to support you!

Would you like to learn more about our products and solutions?
Contact us
Therapy solutions for healthcare professionals
Are you interested in other apheresis procedures?
Plasauto SIGMA device technology
Plasauto SIGMA - the market leader from Japan - for continuous renal replacement therapy and therapeutic apheresis. Suitable even for the youngest and smallest patients! Whether citrate or heparin, outpatient or inpatient - the choice is yours!

The following information is intended for healthcare professionals only.
The information in the section ‚products & therapies‘ is intended to provide explanatory, scientific, and evidence-based answers to medical questions about therapeutic apheresis.
This information does not constitute medical advice. The responsibility for patient care rests with the healthcare professional based on their professional licensure, experience, and knowledge of the patient.